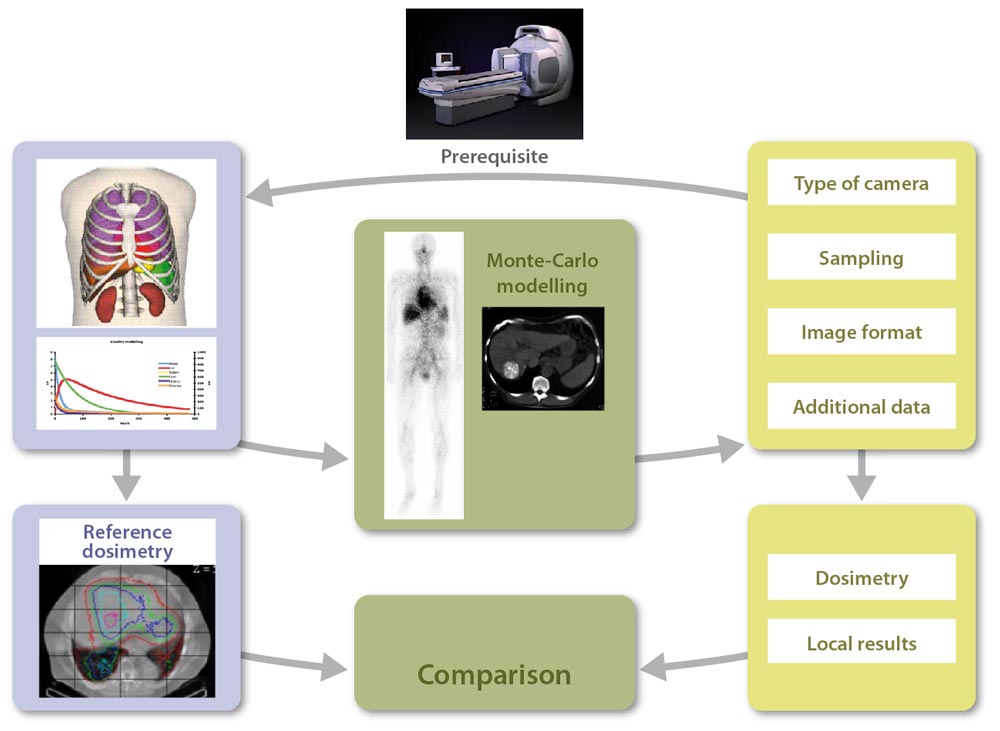
Our lab (hosting lab), creates a virtual patient, a reference dataset {anthropomorphic phantom, pharmacokinetics} defined for all tissues and organs of interest, for a given radiopharmaceutical compound. Monte Carlo modelling is then used for the direct generation of voxel-based reference dosimetry.
Each participating center has to define the data type needed for a dosimetric approach if the study was fully realised locally: planar imaging or SPECT, temporal sampling (number and duration of acquisitions), linked CT images or not, mode of dosimetry calculation, etc.
In addition, they should provide information regarding their gamma camera (type, crystal thickness, etc.), and an example of an experimental image (Jaszczak phantom for example), for us to define their detector model.
We then model the gamma camera used in the participating centre. Modelling validation is done by comparing simulated and experimental images provided by the participating centre. This also allows for testing the import of simulated images in the local image workstations.
Our lab then generates patient images and all additional data required for the dosimetric study (including calibration images), at different times and using a format adapted to the local needs, to obtain a dataset equivalent to what would have been acquired on a real patient.
Scintigraphic images quantification and activity determination are performed by the participating centre, for organs and tissues of interest (liver, kidneys, spleen, lungs, tumours, etc.). The dosimetric study is performed using local resources (commercial or in-house software…).
The participating centre then sends results to the hosting lab to benchmark its approach against the reference. In addition, some intermediate results are transmitted to the hosting lab to allow tracing the different steps of the clinical dosimetry workflow.
The comparison between local results obtained by each participating centre and reference results initially generated by the hosting lab increments a database , thereby allowing the assessment of critical steps in the dosimetry workflow (inducing large variability between centres).